Types of PRP: Which Is Best? The Empire Strikes Back…
We’ve used many types of platelet-rich plasma (PRP) through the years. What we produce in the lab is far more potent than what most practices can accomplish with simple bedside centrifuges. However, what most patients don’t know is that there are different types of PRP. The two main types are red and amber, and which one to use has caused quite a big stir in the orthobiologics community.
What Is PRP?
PRP stands for platelet-rich plasma. The general idea is that you take whole blood from a vein and then concentrate the platelets. Why do this? Platelets have growth factors that act like espresso shots for cells that can repair tissue. Hence, PRP can help stimulate a damaged area that isn’t healing to help repair itself.
A key thing that we have always seen is that the number of platelets in the mix matters. Time and time again, when we’ve tested different types of PRP in the lab, we’ve seen that those with a higher platelet concentration cause the test cells to proliferate (grow) more robustly. Hence, we use high-dose PRP that generally has much higher platelet levels than those produced by a simple bedside centrifuge.
Flexible Lab Platform vs. Little Bedside Machine
At Regenexx, we never want to be backed into a corner by one technology. Meaning, we want to be able to produce whichever orthobiologic concoction has been shown to be the most effective or that we think will help the most. As an example, most providers who offer PRP use a one-size-fits-all bedside machine. This means that this technology usually only produces one type of PRP at one concentration. At Regenexx, we use a flexible lab platform that allows us to produce many different types of platelet-based products at many different concentrations. We also produce advanced platelet lysates, which are growth-factor-rich serum cocktails. Watch my video below for the differences between a bedside machine and a flexible lab platform:
Amber vs. Red PRP
After performing PRP injections for many years, I first got my introduction to the problems with red PRP at a medical conference. A physician approached me after a lecture and asked how we handled the severe flare-ups after injecting PRP into knees including large effusions (fluid-filled knees). In his practice, these had caused hospitalizations in a few of his patients. I was dumbfounded, as I had never seen this happen due to injecting a knee with PRP. Turns out this provider was using red PRP versus the amber type we used. Let’s look at those differences.
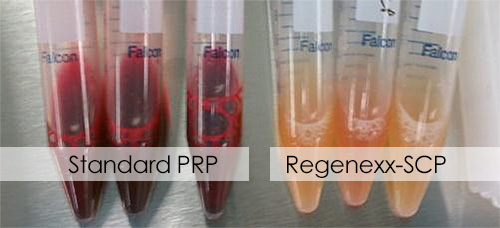
Above I have a picture showing red PRP on the left (standard) versus amber PRP on the right (the type we use at Regenexx). If the PRP preparation is red, this generally means that the red blood cells (RBCs) and white blood cells (WBCs) have been left in the PRP. This is called leukocyte-rich (LR). If the PRP is amber, it’s generally because the PRP has the RBCs and WBCs excluded (or fewer). This is called leukocyte-poor (LP). All of these extra RBCs and WBCs are the reason why most believe that red PRP (LR) produces a much bigger patient flare-up after injection. In essence, the body reacts like there has been a serious injury or infection, as it only usually sees this many RBCs or WBCs in one place during those medical issues.
You should also know that doctors frequently refer to platelet concentration by use of the notation “X.” This means the number of times the platelets are concentrated over what’s in the patient’s whole blood. Hence, a 3X PRP has three times more platelets than whole blood. A 14X PRP has fourteen times, and so on.
Which Is Better?
Causing an inflammatory response in a patient is not always a bad thing, as that provides another bite at the proverbial healing apple. Having said that, in some patients with metabolic syndrome (overweight, high blood pressure, and high triglycerides), this can be like bringing gasoline to a bonfire and lead not to tissue regeneration and repair but unwanted scarring. So which is generally better, red or amber?
A few studies have been done through the years. For these references, see below (bottom of the page). For example, one study found that LR (red) caused a bigger flare-up after the injection and that this was directly related to the number of WBCs. Another found that LR PRP (red) hurt fibroblast cells (the type of cells found in ligaments).
For knee arthritis, multiple studies have shown issues with red PRP. One demonstrated that LR PRP (red) hurt synovial cells and caused inflammation. Another showed that LP (amber) caused better chondrocyte (cartilage cell) proliferation in culture. Finally, a third demonstrated that LP (amber) outperformed LR (red) in knee functional scores when knee arthritis was being treated. In tendon injuries, LR (red) caused more inflammation, but both produced the same improvement in tendon cell numbers (i.e., a stronger tendon).
The Company 510K Dilemma
So this would appear to be settled, right? LP (amber) is better than LR (red), or at least it doesn’t cause a massive flare-up and the results are similar in some applications. However, the problem is that we have companies that are locked into the type of PRP kit (LR vs. LP) they submitted to the FDA for 510K device registration. Unlike someone with an onsite lab that can make either, the doctors that bought these units are locked into that one technology. Given that this research about red vs. amber has been presented at multiple medical conferences and that LP (amber) causes fewer flares than LR (red), the companies that make LR kits and machines have been losing market share to companies that make LP machines. However, in medicine, that just means that scientists who work with companies that make LR devices and related academics have been working overtime to try to spin the story in the opposite direction.
The Empire Strikes Back: Two New Studies
I kind of view this whole dynamic like Star Wars. The rebels (LP—amber) begin to gain a victory over the PRP establishment (LR—red, or the “Empire”). After all, LR machines were the first to hit the market, and up until recently, they held the lion’s share of the PRP market. Then the Empire strikes back with a bevy of studies and KOLs. What is a KOL? It’s pharma speak for a “key opinion leader,” someone who is hired by a company to try and convince doctors to buy their products. Sometimes this is a scientist, sometimes a famous doctor, or sometimes an academic.
Let’s review two new studies that show the pushback against the research already reviewed above.
The First Recent Study
The first study is out of Australia and was published in a high-impact journal. It’s a meta-analysis, which is a research paper that looks at the data presented in other papers and tries to group types of therapies together to get a bigger number of patients than any individual study could muster. The good news is that the study concluded that PRP helps tendons. The bad news is that the author then over-reached by trying to conclude with LR (red) was better than LP (amber) for tendons. Let me explain.
The meta-analysis had 11 studies that used LR PRP (red) with a collective patient n of a whopping 767 patients! The author only had two studies that used what she considered LP PRP (amber), and these studies had only 28 and 25 patients. The first study of 28 patients didn’t actually use PRP, IMHO, because the product is known to barely concentrate platelets over whole blood (1–2X). So we can exclude those 28 patients as most authors believe that a PRP has to have at least 3X concentration. The second study of 25 patients only had 15 patients who got the treatment. Hence, given that the whole purpose of a meta-analysis is to ensure that you have more patients to compare than a single small study could provide, this wasn’t a meta-analysis when it came to comparing LR (red) and LP (amber). From a statistical standpoint, the humongous discrepancy in the number of patients here makes this whole exercise a huge type-two error. What does that mean? Basically, the paper, from the standpoint of comparing LR (red) and LP (amber), isn’t worth the paper it’s written on.
The Second Recent Study
One of the strategies that pharma companies use to gain market share is to use KOLs on the science side. These are usually PhDs who know their field of expertise at a much deeper level than the average physician. Hence, it’s not hard for them to easily confuse doctors and make them believe pretty much anything they want.
One of the companies new to the PRP space is powerhouse Johnson & Johnson (J&J). It now sells a nifty little machine that it calls the PEAK PRP System, which started out life as the Genius Concentration system from Reinvent Biologics. Recently, the CEO of Reinvent posted a paper on LinkedIn written by a J&J company employee that purported to show that LR (red) was dramatically better than LP (amber). The problem with the paper is that it also doesn’t have the data to support the conclusions that LR is better.
The paper compares the PEAK system to ACP (autologous conditioned plasma). The latter is a product of a machine made by Arthrex, which generally has a bigger orthopedic market share in many products than J&J. As discussed above, the problem with ACP is that it’s not really a platelet concentrate. A competitor (Biomet) looked at the platelet content of ACP and found it to be very low.
This new paper then looked at the ability of the serum from the LR PRP (red stuff from the PEAK system) to be able to help tenocytes grow (tendon cells). This was compared to the output from the Arthrex system producing amber colored ACP (which J&J characterized as LP). Not surprisingly, the PEAK system beat the Arthrex system. However, this was a foregone conclusion as the PEAK system had about four times more platelets and a lot more growth factors in the serum. Since more growth factors in all of our in-vitro lab work have always meant better cell growth, the study just proved that having more platelets was better.
The author then went down a rabbit hole of trying to convince the reader that since the ACP had about twice the platelets of whole blood but didn’t do any better than the whole blood in causing tendon cells to grow, this meant that since whole blood had more white blood cells (and other cells), this was the cause of the effect observed. Basically, that the white blood cells and possibly other cells in the mix that were in the red PRP and absent in the amber PRP caused the tendon cells to grow better. While it’s possible that this was the case, to prove that, the research study would have had to selectively add back certain cells to the LP amber PRP and look at cell growth for each condition. That didn’t happen.
In our extensive PRP lab experience, a 2X PRP is not that much better than serum without platelets. Hence, the observed results. Meaning, in this study, having more platelets caused more cell growth.
What’s interesting about ACP is that Arthex published a white paper showing that it had much better ability to cause multiple common orthopedic cell types to proliferate than systems that produced LR PRP (this was published before the PEAK system existed). This only highlights that each company produces its own research that often contradicts the research of other companies. Surprised?
My Thoughts
This deep dive into PRP types this morning was begun by Reinvent Biologics posting the J&J paper on LinkedIn, trying to convince doctors to buy its new PEAK PRP system. Since Regenexx doctors already have labs capable of mixing either LR (red) or LP (amber) PRP, the issue for me was whether the companies could present any data that would compel me to expose my patients to the serious postinjection flare-ups of red PRP. Regrettably, nothing compelling was presented, so we’ll stick with high-dose amber-colored LP PRP.
The upshot? As you can see, the little bedside machine crowd is all locked into producing only one type of PRP. Hence, the companies that make these machines have launched salvo after salvo at each other, trying to convince most doctors who barely understand what they’re reading that the machine they make and what it produces is better. At Regenexx, we’ll always stay above this fray by having a lab platform that can produce whatever is best to help heal our patients. So far, that’s high-dose amber PRP.
References
- Adverse reactions in knee OA joint injections not directly related to WBC concentration, LP PRP outperforms LR PRP.—Am J Sports Med. 2016 Mar;44(3):792–800.
- LR PRP stimulates a pro-inflammatory environment in fibrin scaffolds that hurt fibroblast and osteoblast proliferation. PLoS One. 2015 Mar 30;10(3):e0121713.
- LR resulted in significant synovial cell death and pro-inflammatory mediators in-vitro, whereas LP did not. Am J Sports Med. 2014 May;42(5):1204–10.
- LP caused better chondrocyte proliferation in-vitro. LP caused anabolic ECM production, LR caused catabolism—J Bone Joint Surg Am. 2014 Mar 5;96(5):423–9.
- Knee OA-LP outperformed LR on functional scores—Am J Sports Med. 2016 Mar;44(3):792–800.
- LP caused less tendon inflammation, but similar cellularity-animal model—Am J Sports Med. 2012 Jun;40(6):1274–81

If you have questions or comments about this blog post, please email us at [email protected]
NOTE: This blog post provides general information to help the reader better understand regenerative medicine, musculoskeletal health, and related subjects. All content provided in this blog, website, or any linked materials, including text, graphics, images, patient profiles, outcomes, and information, are not intended and should not be considered or used as a substitute for medical advice, diagnosis, or treatment. Please always consult with a professional and certified healthcare provider to discuss if a treatment is right for you.